GA 2020/0820
Answer
Yes, provided it is kept in the patient’s hospital record and certain other criteria are met.
Context
Doctor A was a respiratory and sleep physician who had been trying to obtain clarity around this question and the associated question answered in GA 2020/0721 on numerous occasions, but had received unclear responses. The question specifically related to weekend cover when doctors are rostered to cover each other’s admitted patients on a rotating basis. Doctor A said that some groups and individuals seem to apply and interpret the requirements differently, which was of concern to her.
Relevant Legislative Provisions
Health Insurance Regulations 2018
Other Relevant Materials
Published academic journal article that provides some analysis of the challenges around compliance with referral requirements and the low levels of legal literacy around the operation of relevant referral law: Wading through Molasses: A qualitative examination of the experiences, perceptions, attitudes, and knowledge of Australian medical practitioners regarding medical billing.
Case law
N/A
Departmental Interpretation
mbsonline.gov.au (accessed 27 July 2020)
“(iii) Hospital referrals.
Private Patients – Where a referral is generated during an episode of hospital treatment for a service provided or arranged by that hospital, benefits will be payable at the referred rate if the account, receipt or assignment form is endorsed ‘Referral within (name of hospital)’ and the patient’s hospital records show evidence of the referral (including the referring practitioner’s signature). However, in other instances where a medical practitioner within a hospital is involved in referring a patient (e.g. to a specialist or a consultant physician in private rooms) the normal referral arrangements apply, including the requirement for a referral letter or note and its retention by the specialist or the consultant physician billing for the service.“
servicesaustralia.gov.au (accessed 26 June 2020)
“Referrals for specialist treatment
Patients can be referred to a specialist or consultant physician for treatment of their condition. The referral must include:
- relevant clinical information about the patient’s condition for investigation, opinion, treatment and/or management
- the date of the referral, and
- the signature of the referring practitioner
Referrals don’t need to be made out to a certain specialist or consultant physician.
Referrers should let patients choose where to present the referral, this also applies to electronic referrals.”
Detailed Reasoning
Like much of Medicare’s enabling legislation, referral law is complex, and as a result, poorly understood. Yet referrals are a critically important component of Medicare billing and one of the key cost control mechanisms in the scheme.
In-hospital referrals have become so badly managed that it is now common for a doctor to have multiple, overlapping, concurrent referrals for the same patient, and for patients to see claims appearing on their Medicare records for services provided by doctors they have never heard of.
Yet hidden deep in the law is an in-hospital referral system that, if properly understood and used correctly, would alleviate a great deal of confusion.
Starting with section 20BA of the Health Insurance Act 1973 (the Act), the law permits confirmation of referral to a specialist to be recorded in a hospital record, a hospital record being defined as follows:
“hospital record” includes the medical records of a person who received medical treatment in the hospital.
Then section 132A of the Act is the linking provision to the Health Insurance Regulations 2018 (regulations), where the details required for valid referrals are set out. There are 3 key regulations that deal with in-hospital referrals.
FIRST: Regulation 58(4) provides:
“Hospital referrals
(4) If the service is rendered to a patient in a hospital who is not a public patient:
(a) paragraphs (2)(b) to (d) do not apply; and
(b) the words “referral within” followed by the name of the hospital are a prescribed particular.“
NOTE: paragraphs (2)(b) to (d) are the paragraphs that require the address or provider number of the referring doctor, the date of the referral and the period of validity. They are not required for in-hospital referrals. However the name of the referring doctor in (2)(a) has not been excluded and is therefore required.
SECOND: Regulation 100 provides:
“100 Requirement to record certain referrals in hospital records
If a referral is for a patient in a hospital who is not a public patient, approval of the referral by the referring practitioner must be included in the hospital records. The approval must be signed by the referring practitioner.“
THIRD: Regulation 102(5) provides:
“Special cases
(5) A referral for a professional service to a patient in a hospital who is not a public patient is valid until the patient ceases to be a patient in the hospital who is not a public patient.“
Bringing these 3 regulations together, it is not necessary or appropriate to create new referrals to and from each other when you are providing inpatient locum cover. To comply with the regulations, when writing a referral for your locum, the following 3 simple steps should be followed:
1. Make an entry in the patient’s hospital record saying something like – “Referred to Doctor B to continue care over the weekend.”
2. Date the entry.
3. Make sure your name is clear and legible, and sign the entry.
Examples and other relevant information
The regulations are designed such that there should only ever be one active referral for a patient in a hospital bed (ideally from the GP or the Director of the Emergency Department) and all other specialists should follow the above steps.
Also, please note that any referral entered in a patient’s hospital record cannot be carried forward and used once the patient has been discharged. Regulation 102(5) provides that in-hospital referrals automatically expire when the patient is discharged.
Using handover sheets is fine (though not necessary unless you prefer them for other reasons), but they must be dated and signed by the person handing over the patient, and stored in the hospital record.
When you are the recipient of an in-hospital referral DO NOT enter the name of your colleague as the referrer on your claims, or the GP or anyone else. All ECLIPSE enabled billing software has an ‘in-hospital’ referral override flag, which is designed specifically for this scenario.
You should also add the word “locum” or “LT” in the service text of your claims. Please read GA 2020/0721 for details of this requirement.
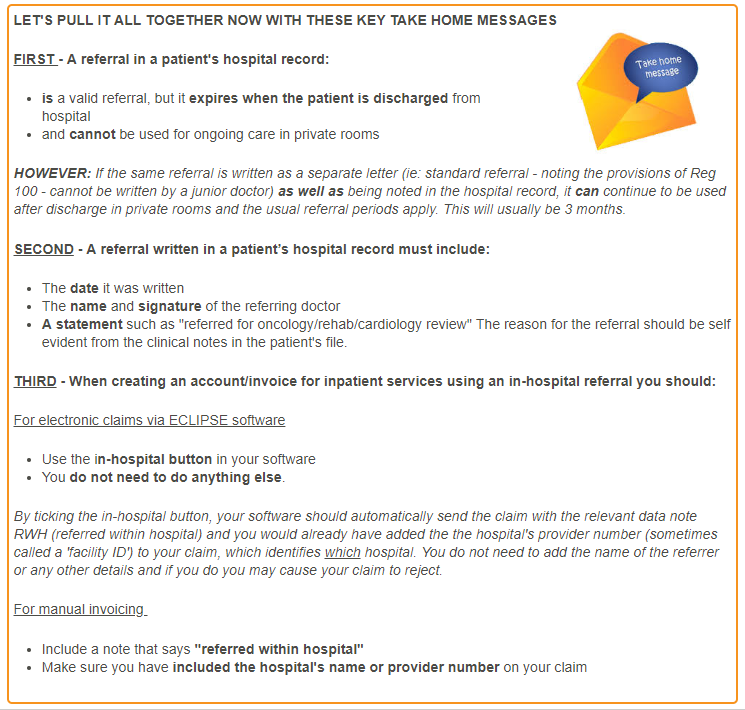
Below is a snapshot from our Rules of Referrals online course that brings the in-hospital requirements together.
Who this applies to
All specialists covering for each other for admitted patients.
Please note, this answer does not apply to outpatients, where different referral regulations apply.
When this applies
Always