GA 2021/0229
Answer
Yes, in our opinion, but not as a modus operandi.
Context
The question posed was: If an ECG is performed during a pre-admission consultation (MBS Item # 17610 or 17615) and the criteria of item number 11714 is met, is it permissible to claim both?
Relevant Legislative Provisions
Health Insurance (General Medical Services Table) Regulations (No. 2) 2020
Health Insurance (Section 3C General Medical Services – Cardiac Services) Determination 2020
Other Relevant Materials
Please read this answer in conjunction with GA 2020/0822
Case law
N/A
Departmental Interpretation
Major changes to cardiac services were introduced on 1 August 2020, based on recommendations made by the MBS Review taskforce. You can read the details and download various fact sheets here.
Detailed Reasoning
To start, let’s review and compare the law describing the item 11714 ECG service, versus Medicare’s interpretation of the law.
Below is the law, which you can also access at this link.
Now let’s review Medicare’s interpretation of the law on the MBS Online website, which you can access at this link.
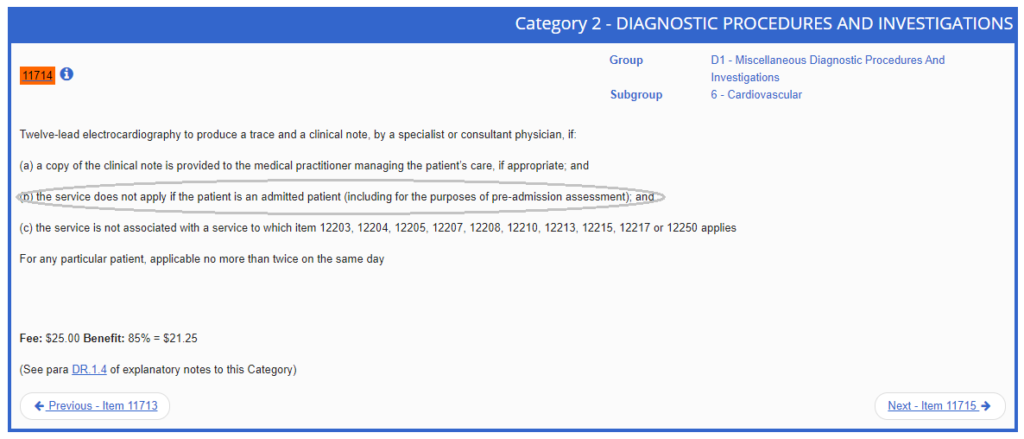
As you will see, an additional point (b), which we have circled for you, has been added to the MBS Online interpretation which is not contained in the law.
The text of point (b) commences with “the service does not apply if the patient is an admitted patient”. This text is largely redundant and unnecessary because the item only attracts an 85% outpatient rebate anyway. So it really just states the obvious.
It is the bracketed text that is troublesome, misaligned with the law and was no doubt the source of confusion for the person asking this excellent question. It states: “(including for the purposes of pre-admission assessment)”
So, we have a situation where the law clearly enables an item 11714 ECG to be claimed for any outpatient, including, by inference, for a pre-admission assessment. But Medicare’s interpretation of the law suggests the opposite. This is unfortunately very common throughout the Medicare scheme.
Applying the law to the scenario posed by the question, let’s step through it:
- Medicare reimburses clinically relevant services. That means the service must be necessary for the treatment of the patient as judged by medical peers.
- If an item 11714 is a clinically relevant service for a non-admitted patient, the starting point is therefore that it can be claimed, provided all legal requirements of the item are met.
- Items 17610 and 17615 are commonly billed pre-anaesthetic consultations and neither is restricted with item 11714 under the law (which, on that point, Medicare concurs). So, to the first part of this question, yes these items can be co-claimed, but…
- Where the law and Medicare diverge is on the issue of clinical relevance. The law has left open the issue of why a medical practitioner may decide that an ECG item 11714 is clinically relevant. Whereas, Medicare is basically saying that pre-admission assessments never meet the requirements for clinical relevance.
- Both medical practitioners and Medicare are subject to the law – neither are above it. Further, should this issue ever come before a court, the judge will apply the law, not the MBS. However, the Department (Medicare) is sending a fairly clear message by it’s insertion of point (b) that doing routine pre-admission ECGs on every patient prior to the patient being admitted for a procedure under anaesthetic, is not something they support.
- You do not want to be the first person challenging this in the Federal Court, so the best advice is therefore that while in our opinion there is no legal barrier to co-claiming these services in your pre-anaesthetic/pre-admission clinic, we do not recommend you adopt it as a modus operandi and do ECGs on every patient. Remember the basic principle of clinical relevance, which is directly linked to necessity. If patients are fit and healthy and there is no clinical indication or necessity for an ECG, don’t do one. However, for patients whose health status clearly does warrant an ECG prior to being admitted for surgery, then go ahead, but document comprehensively explaining why an ECG was clinically indicated for every such patient.
Examples and other relevant information
Regulation 6(2) of the Cardiac Services Determination has the effect of including item 11714 in the supervision rules set out in Regulation 1.2.11(1) of the General Medical Services Table. Which means the service can be provided by someone other than a medical practitioner (usually a nurse) under the supervision of the medical practitioner.
Who this applies to
All specialists and consultant physicians.
When this applies
Since 1 August 2020